- Medicines
- Personal Care
- Skin Cream
- Sunscreen
- Face Wash
- Skin and Body Soap
- Acne Care
- Body Lotions
- Moisturising Lotion
- Moisturising Cream
- Mosquito Repellent
- Moisturising Gel
- Body Wash
- Hair Oils
- Hair Shampoo
- Hair Conditioners
- Hair Supplements
- Hair Colour
- Hair Serum
- Hair Mask
- Hair Solutions
- Baby Diapers and Wipes
- Baby Lotion and Moisturising Cream
- Baby Bath Essentials
- Baby Skin Care
- Baby and Infant Food
- Baby Healthcare
- Women Multivitamins
- Ovulation Test Kit and Women Intimate Care
- Sanitary Pads
- Nutritional Drinks
- Condoms
- Lubricants
- Massage Gels
- Personal Body Massagers
- Men Performance Booster
- Sexual Health Supplements
- Massage Oils
- Ayurveda
- Tooth Paste
- Mouth Ulcer Gel
- Mouthwash
- Toothache and Gum Pain
- Tooth Brush
- Gargle Solution
- Orthopaedic Supports
- Adult Diapers
- Footwear
- Mobility and Support Accessories
- Urinary Support and Care
- Health Conditions
- Bone and Joint Care
- Digestive Care
- Eye Care
- Pain Relief
- Smoking Cessation
- Liver Care
- Stomach Care
- Cold and Cough
- Heart Care
- Kidney Care
- Piles, Fissures & Fistula
- Respiratory Care
- Mental Wellness
- Derma Care
- Pre and Probiotics
- Acidity
- Gas
- Constipation
- Loose Motion/Diarrhoea
- Digestive Fibres
- Digestive Enzymes
- Eye Lubricant Drops
- Lens Solution
- Safety Eye Wear
- Eye Cream
- Eye Vitamins and Supplements
- Eye Drops
- Eye Ointment and Gel
- Nicotine Patch
- Nicotine Gum
- Nicotine Lozenges
- Cough Syrups
- Chest Rubs and Balms
- Nasal Spray
- Lozenges
- Inhalant Capsules
- Cold and Cough Tablets
- Vitamins & Supplements
- Diabetes Care
- Healthcare Devices
- Homeopathic Medicine
- Health Guide
Oesophageal Cancer
Oesophageal cancer is a malignant tumour arising from the mucosal epithelium of the oesophagus. Common presenting features include progressive dysphagia (initially for solids then liquids), unintentional weight loss, odynophagia, chest or retrosternal discomfort, and voice change or chronic cough when local invasion or recurrent laryngeal nerve involvement occurs. Management is stage-dependent and commonly involves a multidisciplinary approach combining endoscopic therapy for very early lesions, surgery (oesophagectomy) for resectable disease, and systemic therapies (neoadjuvant/adjuvant chemotherapy or chemoradiotherapy, targeted therapy, and immunotherapy) or palliation for advanced disease.
Last updated on : 05 May, 2026
Read time : 14 mins
Overview of Disease
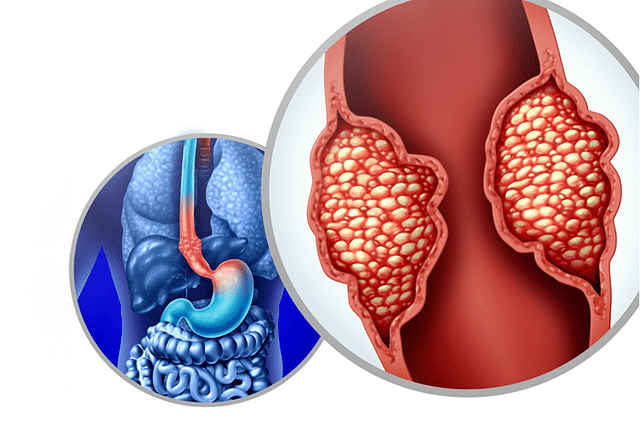
Oesophageal cancer is a type of cancer that originates in the oesophagus, the muscular tube responsible for transporting food and liquid from the throat to the stomach. This cancer occurs when malignant cells form in the tissues of the oesophagus, leading to the development of a tumour. It is important to note that oesophageal cancer can start at any point along the length of the oesophagus. Care should be coordinated by a multidisciplinary team (MDT) including a thoracic/upper gastrointestinal surgeon, medical oncologist, radiation oncologist, gastroenterologist, radiologist, pathologist, dietitian, and palliative care specialists to individualise staging, treatment sequencing, and supportive care. In this article, we will discuss the stages, types, and risk factors associated with oesophageal cancer.
What is Oesophageal Cancer?
Oesophageal cancer is a malignancy arising from the oesophageal epithelium. There are two predominant histologic subtypes: squamous cell carcinoma (SCC), typically arising in the mid to upper oesophagus and strongly associated with tobacco and alcohol exposure and certain environmental factors; and adenocarcinoma, which most often arises in the distal oesophagus or at the oesophagogastric junction (OGJ) and is associated with Barrett’s oesophagus and chronic gastro-oesophageal reflux disease (GERD). Other, less common histologies (eg, small cell carcinoma, lymphoma, sarcoma) occur but represent a small minority. Understanding the stages of oesophageal cancer is essential for determining the appropriate treatment and prognosis.
Key Factors about Oesophageal Cancer
| Category | Details |
| Also Referred as | Oesophagus cancer, Oesophageal carcinoma |
| Commonly Occurs In | People in their 60s and 70s, more common in men than women |
| Affected Organ | Oesophagus |
| Type | Squamous cell carcinoma, adenocarcinoma, sarcoma, small cell carcinoma, lymphoma |
| Common Signs | Difficulty swallowing (dysphagia), weight loss, chest pain, coughing, hoarseness |
| Consulting Specialist | Multidisciplinary team (thoracic/upper GI surgeon, medical oncologist, radiation oncologist, gastroenterologist, radiologist, pathologist, dietitian, palliative care). |
| Treatement Procedures | Endoscopic therapy (for selected T1a lesions), oesophagectomy (open, minimally invasive), chemoradiotherapy (definitive or neoadjuvant), systemic chemotherapy, targeted therapy, immunotherapy, and palliative procedures (stenting, dilatation, feeding access). |
| Managed By | 5-fluorouracil (5-FU), capecitabine, cisplatin, oxaliplatin, paclitaxel, docetaxel, pembrolizumab, nivolumab, trastuzumab, ramucirumab |
| Mimiciking Condition | Gastro-esophageal reflux disease (GERD), other swallowing disorders |
Types of Oesophageal Cancer
Oesophageal cancer is primarily classified into two types based on the specific cells involved in the development of the tumour. These types are:
- Squamous cell carcinoma: This type of oesophageal cancer arises from the squamous cells that line the inner surface of the oesophagus. It is most commonly found in the upper or middle parts of the oesophagus and is strongly associated with heavy alcohol consumption and smoking.
- Adenocarcinoma: This type of oesophageal cancer develops from the gland cells in the oesophagus, particularly in the lower portion near the stomach. It is associated with Barrett's oesophagus and gastro-oesophageal reflux disease (GERD). Adenocarcinomas most commonly arise in a background of Barrett’s oesophagus (intestinal metaplasia), and the rising incidence of distal oesophageal adenocarcinoma in Western countries is linked to GERD, obesity, and metabolic risk factors.
Early Signs of Oesophageal Cancer
Early signs and symptoms may be subtle. Common presenting features include progressive dysphagia (initially for solids, then for liquids), odynophagia, unexplained weight loss, persistent or progressive hoarseness (if recurrent laryngeal nerve involvement), and chronic cough. Early lesions (Tis/T1a) can be asymptomatic and detected on surveillance for Barrett’s oesophagus.
Symptoms of Oesophageal Cancer
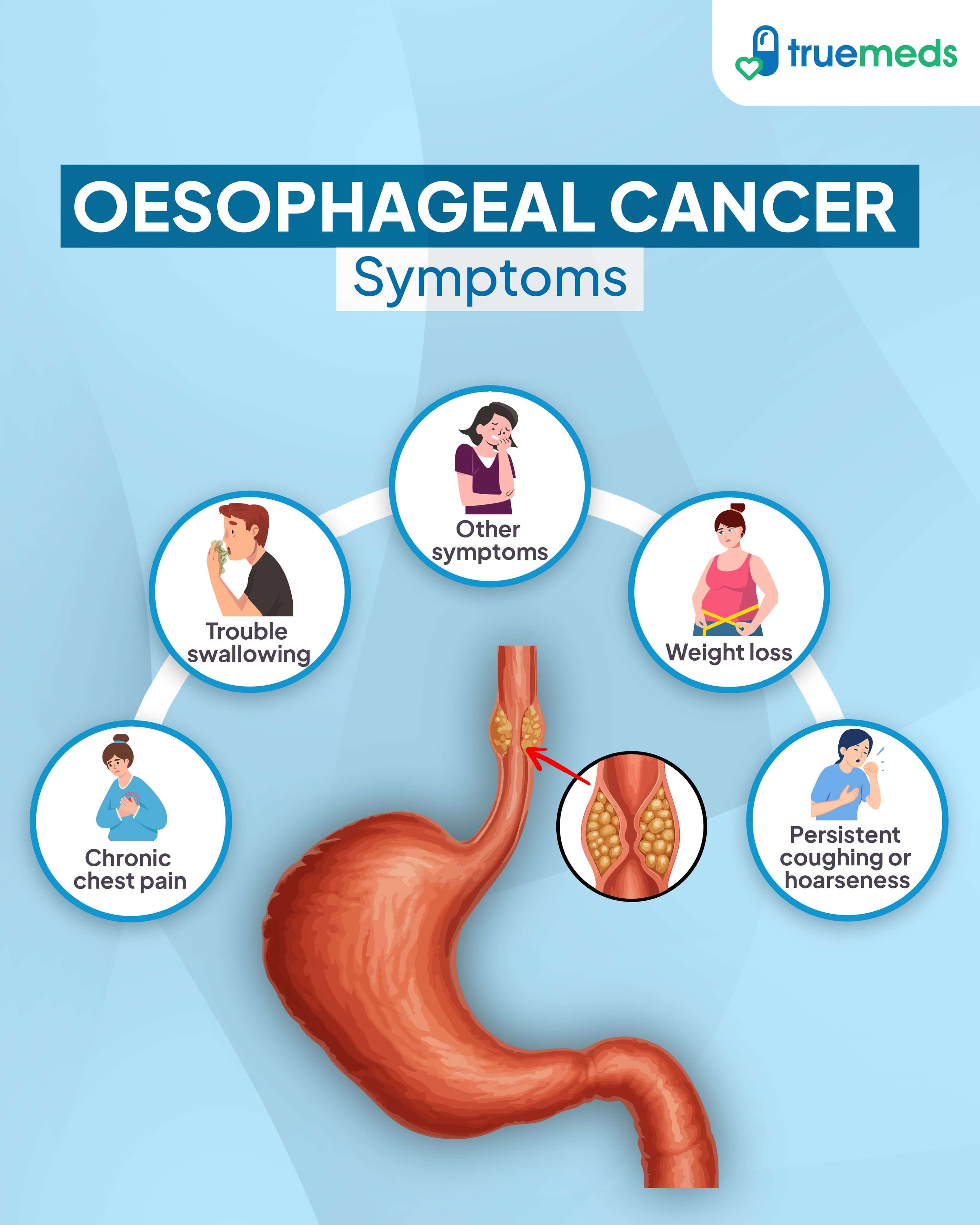
Oesophageal cancer symptoms often remain unnoticeable until the cancer reaches an advanced stage. As the disease progresses, individuals may experience:
- Trouble swallowing: Difficulty swallowing solid foods, liquids, or even saliva can lead to choking or an inability to swallow.
- Chronic chest pain: Pain in the middle of the chest that worsens over time, especially when swallowing, is a common symptom.
- Weight loss: Unexplained weight loss due to reduced appetite or difficulty eating may occur.
- Persistent coughing or hoarseness: Developing a hoarse voice or a cough that does not improve can be a sign of oesophageal cancer.
- Other symptoms: Vomiting, bone pain, and upper gastrointestinal bleeding, which may present as black, tarry, foul-smelling stools and anaemia.
Stages of Oesophageal Cancer
Staging uses the AJCC/UICC TNM system (8th edition) and combines depth of tumour invasion (T), regional lymph node status (N), and distant metastasis (M) to derive stage groups (NCCN, 2024). Key practical points for readers:
- Stage 0 (Tis): High-grade dysplasia/carcinoma in situ limited to the mucosa; often managed with endoscopic therapy in suitable patients.
- Stage I (T1): Tumour invades lamina propria, muscularis mucosae, or submucosa (T1a vs T1b). T1a (mucosal) lesions may be amenable to endoscopic mucosal resection/ablative therapy; T1b (submucosal) lesions have higher nodal risk and often require oesophagectomy or combined therapy.
- Stage II–III (T2–T3 and/or regional N+): Locally advanced disease often managed with multimodality therapy, typically neoadjuvant chemoradiotherapy (or perioperative chemotherapy for adenocarcinoma, depending on location and protocol) followed by resection when appropriate. Definitive chemoradiation is an option for unresectable disease or for patients unfit for surgery.
- Stage IV (M1): Distant metastatic disease, systemic therapy (chemotherapy ± targeted therapy ± immunotherapy) and palliative interventions; select cases with oligometastatic disease may be considered for local therapy within clinical trials.
Causes of Oesophageal Cancer
Oesophageal cancer develops when mutations occur in the DNA of cells in the oesophagus, leading to uncontrolled cell growth. Several factors can increase the risk of developing this type of cancer:
- Chronic heartburn or acid reflux: Conditions like gastro-oesophageal reflux disease (GERD) can cause damage to the lining of the oesophagus over time.
- Barrett's oesophagus: This condition, which develops in some people with GERD, increases the risk of adenocarcinoma, a type of oesophageal cancer.
- Smoking and heavy alcohol consumption: Both habits are closely associated with the development of squamous cell carcinoma, another form of oesophageal cancer.
- Achalasia: This rare disorder affecting the muscles in the lower oesophagus can increase the risk of squamous cell carcinoma.
Risk Factors
While oesophageal cancer can affect anyone, certain factors can elevate the risk of developing this condition:
- Median age at diagnosis is ~65–70 years in many series; risk increases with age (most patients are older adults). Male sex and geographic/ethnic variations influence histologic predominance (eg, SCC is more common in parts of Asia/Africa; adenocarcinoma is more common in Western countries).
- Male gender
- Central obesity
- A diet low in fruits and vegetables
- Chronic acid reflux and Barrett's oesophagus
- Achalasia, a condition that affects the muscles of the oesophagus
Who's at Risk?
Certain groups of people may be at a higher risk of developing oesophageal cancer:
- People with chronic acid reflux or GERD
- Individuals with Barrett's oesophagus
- Smokers and heavy alcohol drinkers
- Those with achalasia
- Older adults, particularly those over 55 years old
- Men
- People who are overweight or obese
- Individuals with a diet low in fruits and vegetables and high in processed meats
- Those who have undergone previous radiation therapy to the chest or upper abdomen
Complications
Oesophageal cancer and its treatment can lead to several complications that significantly impact the patient's quality of life and survival. Some of the postoperative complications include:
- Anastomotic leak: A serious complication where a leak occurs at the junction of the oesophagus and the stomach or bowel, which can lead to mediastinitis and sepsis, and requires immediate treatment.
- Breathlessness and chest infections: Patients may experience breathlessness and are at risk of chest infections, including pneumonia.
- Voice changes: May result from injury to the recurrent laryngeal nerve during surgery or from tumour invasion; can be temporary or permanent.
- Perioperative cardiopulmonary complications: Conditions such as atrial fibrillation, pneumonia, and respiratory failure are common after oesophagectomy and are significant contributors to postoperative morbidity and mortality.
- Functional gastric emptying disorder: Some patients may experience gastric emptying disorders due to the resection of part of the stomach, leading to delayed emptying of stomach contents.
- Eating problems and weight loss: Many patients experience difficulties eating, leading to weight loss, which may necessitate a feeding tube and dietary adjustments.
Other complications of oesophageal cancer include obstruction, where the tumour can obstruct the oesophagus, making swallowing difficult; aspiration, where food or liquid enters the airway; and reflux, where surgery can cause gastro-oesophageal reflux, leading to symptoms like heartburn.
Prevention of Oesophageal Cancer
Certain lifestyle changes can significantly reduce the risk of developing this condition. Some of the key steps for oesophageal cancer prevention include:
- Maintaining a healthy weight: Being overweight or obese increases the risk of oesophageal cancer, particularly adenocarcinoma.
- Eating a balanced diet: A diet rich in fruits, vegetables, and whole grains may help reduce the risk of oesophageal cancer.
- Limiting alcohol consumption: Excessive alcohol intake is a significant risk factor for oesophageal cancer, especially squamous cell carcinoma.
- Quitting smoking: Smoking is a major risk factor for both types of oesophageal cancer, and quitting can significantly reduce the risk.
- Managing acid reflux: Chronic acid reflux, or gastro-oesophageal reflux disease (GERD), can increase the risk of oesophageal adenocarcinoma. Treating GERD with lifestyle changes and medication can help prevent the development of Barrett's oesophagus, a precancerous condition.
- Screening for Barrett's oesophagus: Targeted endoscopic screening may be considered in high-risk individuals with chronic GERD and additional risk factors, which can help detect precancerous changes early. Patients with chronic GERD and confirmed Barrett’s oesophagus should undergo guideline-directed endoscopic surveillance and risk-stratified management (including endoscopic therapy for confirmed dysplasia) to reduce progression to adenocarcinoma (ESMO, 2022).
Diagnosis & Tests
The following diagnostic tests and procedures are commonly used to diagnose oesophageal cancer:
- Endoscopy with biopsy: mandatory to obtain histologic diagnosis and biomarker testing (HER2, PD-L1 by IHC as indicated).
- Endoscopic ultrasound (EUS): best modality for assessing depth of invasion (T stage) and regional nodal evaluation, where available, especially for curative-intent cases.
- Cross-sectional imaging (contrast chest/abdomen CT) and PET-CT: for detection of distant disease and nodal metastases and for staging before curative therapy; PET-CT is preferred for systemic staging in many guidelines (ESMO, 2022).
- Staging laparoscopy: may be considered for distal oesophageal/OGJ adenocarcinoma to detect occult peritoneal disease before planned resection.
- Biopsy: histology and biomarker testing (HER2 for adenocarcinoma; PD-L1 for later therapeutic decisions) should be performed on diagnostic tissue.
- MSI/MMR testing: mismatch repair (MMR) or microsatellite instability (MSI) testing may be performed in selected cases to guide immunotherapy.
A multidisciplinary review of imaging and histopathology is essential to plan therapy.
Treatment & Management
The management of oesophageal cancer involves a multidisciplinary approach tailored to the stage and type of the cancer. The treatment options may include:
- Surgery: For early-stage oesophageal cancer, endoscopic mucosal resection (EMR) or oesophagectomy may be performed.
- Chemotherapy: Used alone or in combination with other treatments, chemotherapy can be given before surgery (neoadjuvant), after surgery (adjuvant), or to relieve symptoms in advanced cases (palliative).
- Radiation therapy: Radiation can be used alone or combined with chemotherapy (chemoradiation) for unresectable tumours or before surgery.
- Immunotherapy: Checkpoint inhibitors like pembrolizumab and nivolumab are used in selected settings based on PD-L1 expression, histology, and treatment context, often in combination with chemotherapy.
- Targeted therapy: Trastuzumab can be added to chemotherapy for HER2-positive tumours.
- Palliative care: Interventions such as endoscopic stenting, intraluminal brachytherapy, and supportive care help manage symptoms and improve quality of life in advanced cases.
The stage of oesophageal cancer is a key determinant of the treatment approach:
- Stage 0 (Tis)/Selected T1a: Endoscopic therapy (endoscopic mucosal resection ± ablation) or oesophagectomy depending on lesion characteristics and patient fitness.
- T1b or node-positive early disease: Surgery (oesophagectomy) and/or combined modality therapy depending on histology and risk features; MDT discussion required.
- Locally advanced (most Stage II–III): Multimodality therapy is standard. For many centres, the preferred approach for resectable disease is neoadjuvant chemoradiotherapy (eg, CROSS regimen) followed by surgery, or perioperative chemotherapy regimens for adenocarcinoma, depending on local protocols and tumour location. Definitive chemoradiotherapy is an alternative for unresectable disease or for patients who are not surgical candidates (NCCN, 2024).
- Adjuvant therapy: For patients with residual pathologic disease after neoadjuvant chemoradiotherapy and R0 resection, adjuvant nivolumab is an approved option to improve disease-free survival in selected patients (per the CheckMate 577 trial).
- Stage IV / Metastatic: Systemic chemotherapy is the primary treatment; HER2-positive adenocarcinomas may receive trastuzumab in combination with chemotherapy; PD-1 inhibitors (eg, pembrolizumab) have approved indications in selected PD-L1-positive metastatic disease and are used in combination with chemotherapy in some first-line settings. Palliative interventions (endoscopic stent, brachytherapy, feeding access) address dysphagia and nutrition.
Immunotherapy and targeted therapy
Checkpoint inhibitors (nivolumab, pembrolizumab) have defined roles in resected disease (adjuvant nivolumab for residual disease after neoadjuvant chemoradiotherapy) and in selected metastatic settings (pembrolizumab combined with chemotherapy for PD-L1 positive tumours in some indications). Use of CTLA-4 inhibitors (eg, ipilimumab) is investigational or limited to specific combinations within clinical trials; they are not routine monotherapy for oesophageal cancer. Selection of targeted and immune agents should be guided by histology (adenocarcinoma vs SCC), biomarker testing (HER2, PD-L1, MSI), and guideline recommendations.
Medications for Oesophageal Cancer
The treatment of oesophageal cancer often involves a multimodal approach, where medications play a crucial role in shrinking tumours, preventing spread, and improving survival outcomes. The choice of medicines depends on the type of cancer (squamous cell carcinoma or adenocarcinoma), stage, patient's overall health, and tumour-specific biomarkers.
- Fluoropyrimidines: 5-FU (infusional), capecitabine (oral prodrug).
- Platinum agents: cisplatin, oxaliplatin. (Carboplatin may be used when cisplatin is contraindicated.)
- Taxanes: paclitaxel, docetaxel.
- Irinotecan, epirubicin: used in some regimens or later lines.
- Targeted therapy: trastuzumab for HER2-positive adenocarcinoma; ramucirumab in the second-line setting for gastro-oesophageal adenocarcinoma. Zolbetuximab (CLDN18.2-targeted therapy) has demonstrated clinical benefit and is being introduced into clinical practice in selected settings.
- Immunotherapy: nivolumab (adjuvant for residual disease after neoadjuvant chemoradiotherapy in resected patients) and pembrolizumab for selected PD-L1-positive metastatic settings per trial evidence and approvals. Ipilimumab is not a routine monotherapy and is primarily used in trial combinations (Kelly et al., 2021).
Supportive medications (antiemetics, PPIs, analgesics, nutritional supplements) should be used per standard oncology supportive care protocols.
When to See a Doctor?
It is essential to consult a doctor if you experience any symptoms suggestive of oesophageal cancer, such as difficulty swallowing (dysphagia), unintentional weight loss, chest pain, hoarseness, or chronic cough, or signs of gastrointestinal bleeding (such as vomiting blood or passing black stools). Early detection and prompt treatment can significantly improve the prognosis of oesophageal cancer. Seek urgent assessment if dysphagia progresses rapidly, there is evidence of upper GI bleeding, unintentional rapid weight loss, or new onset of odynophagia. Early referral for endoscopic evaluation is recommended for persistent red-flag symptoms.
Key Takeaways
- Oesophageal cancer is a malignant tumour that develops in the oesophagus, the tube connecting the throat to the stomach.
- The two main types of oesophageal cancer are adenocarcinoma and squamous cell carcinoma.
- Risk factors for oesophageal cancer include chronic acid reflux, smoking, alcohol abuse, obesity, and a diet low in fruits and vegetables.
- Symptoms of oesophageal cancer may include difficulty swallowing, weight loss, chest pain, hoarseness, and chronic cough.
- Diagnosis of oesophageal cancer involves endoscopy, biopsy, and imaging tests like CT, PET, and endoscopic ultrasound.
- Treatment for oesophageal cancer depends on the stage and type of the cancer and may include surgery, chemotherapy, radiation therapy, immunotherapy, and targeted therapy.
- Early detection and treatment of oesophageal cancer can significantly improve outcomes and survival rates.
FAQs
Is cancer in the oesophagus curable?
How long can a person live with oesophageal cancer?
Is oesophageal cancer curable at stage 4?
Does oesophageal cancer spread quickly?
What can be mistaken for oesophageal cancer?
What are symptoms of stage 1 oesophageal cancer?
How to check for oesophageal cancer?
What is the difference between oesophageal ulcer & cancer?
References
- Kelly, R. J., Ajani, J. A., Kuzdzal, J., Zander, T., Van Cutsem, E., Piessen, G., ... & Wang, J. (2021). Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. The New England Journal of Medicine, 384(13), 1191–1203. https://doi.org/10.1056/NEJMoa2032125.
- Obermannová, R., Babic, B., Arnold, D., Borg, C., Brunner, T. B., Lordick, F., ... & ESMO Guidelines Committee. (2022). ESMO Clinical Practice Guideline: Oesophageal cancer. Annals of Oncology, 33(9), 810–830. https://doi.org/10.1016/j.annonc.2022.06.001
- National Comprehensive Cancer Network (NCCN). (2024). NCCN Clinical Practice Guidelines in Oncology: Esophageal and Esophagogastric Junction Cancers. Version 3.2024. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1433.
- Wang, Y., StatPearls Authors. (2024). Esophageal Cancer. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK459267/.
- National Cancer Institute. (2024/2025). Esophageal Cancer Treatment (PDQ®)–Health Professional Version. National Institutes of Health. https://www.cancer.gov/types/esophageal/hp/esophageal-treatment-pdq
Check Related Salts
Latest health articles

Top Health Essentials






























Disclaimer
Top-Selling Medicines:
...View more
Top-OTC medicines:
...View more
Company
About UsHealth ArticleHealth StoriesHealth LibraryDiseases & Health ConditionsAyurvedaUnderstanding Generic MedicinesAll MedicinesAll BrandsNeed HelpFAQSecuritySavings CalculatorAdvertise with UsSubscribe
Registered Office Address
Grievance Officer
Download Truemeds
Contact Us
Our customer representative team is available 7 days a week from 9 am - 9 pm.
v4.28.5
2026 - Truemeds | All rights reserved. Our content is for informational purposes only. See additional information.
Our Payment Partners

