- Medicines
- Personal Care
- Skin Cream
- Sunscreen
- Face Wash
- Skin and Body Soap
- Acne Care
- Body Lotions
- Moisturising Lotion
- Moisturising Cream
- Mosquito Repellent
- Moisturising Gel
- Body Wash
- Hair Oils
- Hair Shampoo
- Hair Conditioners
- Hair Supplements
- Hair Colour
- Hair Serum
- Hair Mask
- Hair Solutions
- Baby Diapers and Wipes
- Baby Lotion and Moisturising Cream
- Baby Bath Essentials
- Baby Skin Care
- Baby and Infant Food
- Baby Healthcare
- Women Multivitamins
- Ovulation Test Kit and Women Intimate Care
- Sanitary Pads
- Nutritional Drinks
- Condoms
- Lubricants
- Massage Gels
- Personal Body Massagers
- Men Performance Booster
- Sexual Health Supplements
- Massage Oils
- Ayurveda
- Tooth Paste
- Mouth Ulcer Gel
- Mouthwash
- Toothache and Gum Pain
- Tooth Brush
- Gargle Solution
- Orthopaedic Supports
- Adult Diapers
- Footwear
- Mobility and Support Accessories
- Urinary Support and Care
- Health Conditions
- Bone and Joint Care
- Digestive Care
- Eye Care
- Pain Relief
- Smoking Cessation
- Liver Care
- Stomach Care
- Cold and Cough
- Heart Care
- Kidney Care
- Piles, Fissures & Fistula
- Respiratory Care
- Mental Wellness
- Derma Care
- Pre and Probiotics
- Acidity
- Gas
- Constipation
- Loose Motion/Diarrhoea
- Digestive Fibres
- Digestive Enzymes
- Eye Lubricant Drops
- Lens Solution
- Safety Eye Wear
- Eye Cream
- Eye Vitamins and Supplements
- Eye Drops
- Eye Ointment and Gel
- Nicotine Patch
- Nicotine Gum
- Nicotine Lozenges
- Cough Syrups
- Chest Rubs and Balms
- Nasal Spray
- Lozenges
- Inhalant Capsules
- Cold and Cough Tablets
- Vitamins & Supplements
- Diabetes Care
- Healthcare Devices
- Homeopathic Medicine
- Health Guide
Hyperemesis gravidarum
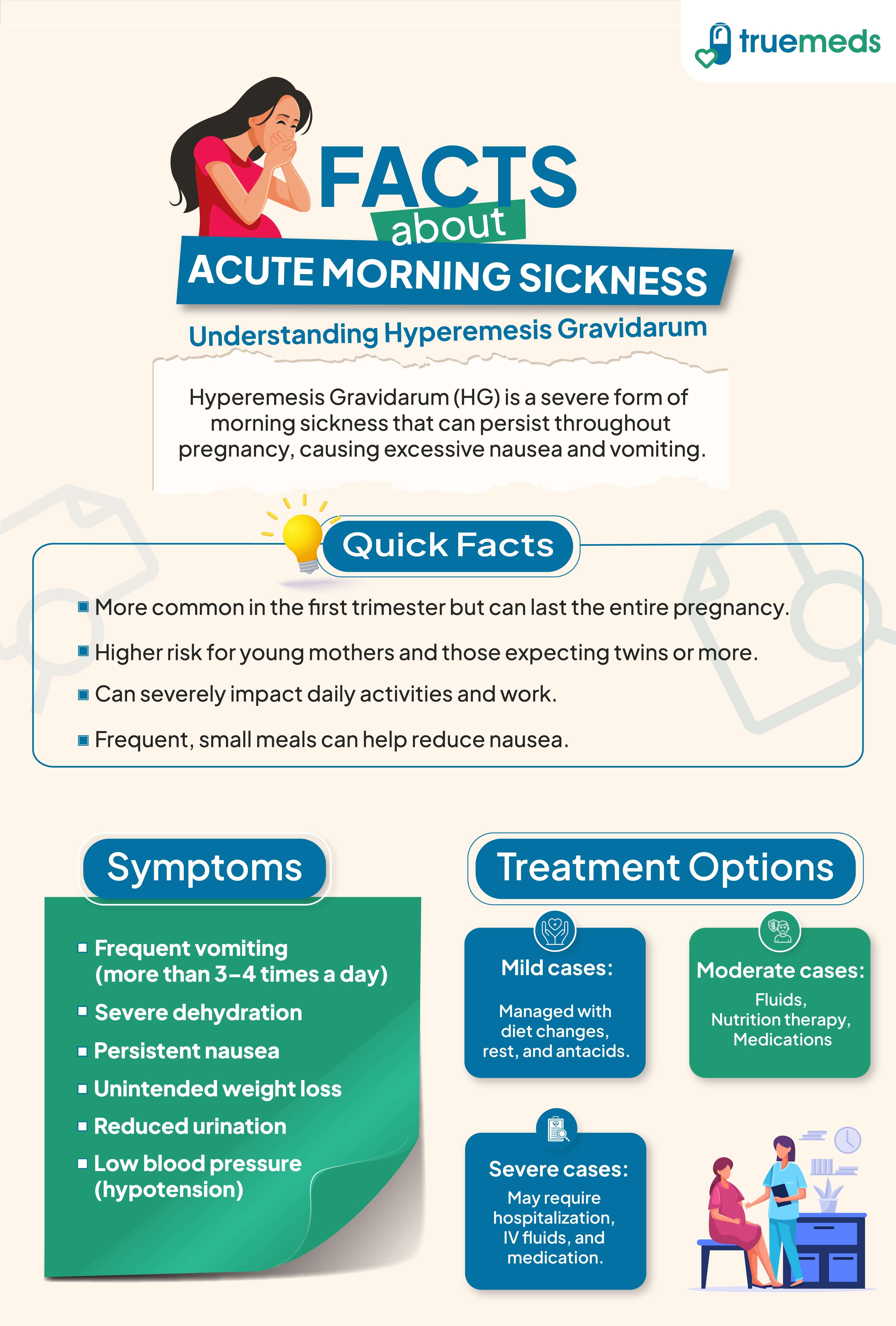
Hyperemesis gravidarum (HG) is a severe form of morning sickness during pregnancy, characterised by intense nausea, vomiting, and potential dehydration. Unlike typical morning sickness, HG can persist beyond the first trimester and may lead to weight loss, electrolyte imbalances, and other complications (Jennings, 2023). Prompt diagnosis and treatment are crucial for managing symptoms and ensuring the well-being of both the mother and the baby.
Last updated on : 06 May, 2026
Read time : 9 mins

Overview of Disease
Pregnancy is a time of significant physical and emotional changes for women, and while some discomfort is expected, certain conditions can greatly impact a woman's quality of life. One such condition is hyperemesis gravidarum, a severe form of morning sickness that affects a small percentage of pregnant women. Expectant mothers need to be aware of this condition, its symptoms, and when to seek medical attention to prevent potential complications.
What is Hyperemesis Gravidarum?
Hyperemesis gravidarum (HG) is a condition in pregnancy where you have severe and constant nausea and vomiting. It can cause weight loss and dehydration. HG is sometimes known as extreme morning sickness.
Key Factors about Hyperemesis gravidarum
| Category | Details |
| Also Referred as | Nausea - hyperemesis, Vomiting - hyperemesis, Morning sickness - hyperemesis |
| Commonly Occurs In | Pregnant women, especially those with multiple pregnancies or a history of HG |
| Affected Organ | Systemic involvement, primarily gastrointestinal symptoms, with secondary effects on the kidneys, liver, and metabolic function due to dehydration and electrolyte disturbances. |
| Type | Severe pregnancy complication |
| Common Signs | Severe, persistent nausea and vomiting, weight loss (>5% of pre-pregnancy weight), dehydration, constipation, excessive salivation |
| Consulting Specialist | Obstetrician, Gastroenterologist |
| Treatement Procedures | Intravenous fluids, antiemetics (e.g., pyridoxine, metoclopramide), temporary suspension of oral intake, and vitamin and electrolyte repletion |
| Managed By | Healthcare providers, including obstetricians and gastroenterologists |
| Mimiciking Condition | Urinary tract infection, gastroenteritis, thyroid disease, multiple pregnancy, molar pregnancy, typical nausea and vomiting of pregnancy |
Symptoms of Hyperemesis gravidarum
Hyperemesis gravidarum (HG) usually starts in the first trimester of pregnancy, around six weeks in. It can last for weeks, months, or even until birth. The symptoms can be very strong and may stop you from doing your daily activities.
Common symptoms of hyperemesis gravidarum:
- Severe nausea
- Recurrent, intractable vomiting that may occur multiple times per day and impairs oral intake.
- Losing more than 5% of your pre-pregnancy weight
- Being unable to keep food or drinks down
- Dehydration
- Dizziness or feeling lightheaded
- Urinating less than usual
- Extreme tiredness
- Fainting
- Headaches
Less common symptoms:
- Low blood pressure
- Fast heart rate
- Dry skin
- Confusion
- Jaundice (rare; may occur secondary to severe dehydration or prolonged vomiting leading to transient hepatic dysfunction).
- A rare neurological complication called Wernicke encephalopathy (due to thiamine deficiency), which may progress if untreated
Causes of Hyperemesis gravidarum
The exact cause is multifactorial and not fully understood. Contributing mechanisms include elevated hCG levels, genetic predisposition, increased sensitivity to pregnancy-related hormones, and emerging evidence implicating the placenta-derived hormone GDF15 as a major driver of HG severity (Fejzo et al., 2024)
Risk Factors
While any pregnant woman can develop hyperemesis gravidarum, certain factors may increase your risk, including:
- A previous history of HG in past pregnancies
- Carrying twins or multiples
- Having a genetic predisposition, particularly if your mother or sister suffered from HG (suggesting the condition may run in families)
- Being prone to motion sickness
Other associated factors may include a history of migraines, motion sickness, or high sensitivity to hormonal changes. Chronic medical conditions (e.g., renal or hepatic disorders) are not established risk factors for HG itself but may worsen tolerance to vomiting (Fejzo et al., 2024).
Prevention of Hyperemesis gravidarum
Preventing hyperemesis gravidarum (HG) with complete certainty is not currently possible. Although there are no known methods to entirely prevent HG, some steps can be taken to potentially reduce its severity or prepare for its impact. Recurrence risk is high, with studies reporting rates of approximately 15–80% depending on diagnostic criteria and severity, but the exact recurrence probability varies across populations. Taking a multivitamin containing vitamin B6 before getting pregnant may help reduce the severity of symptoms. Early, pre-emptive use of vitamin B6 supplements and first-line medications has shown effectiveness in preventing the deterioration of HG symptoms. Maintaining a healthy diet rich in nutrient-dense foods and ensuring adequate levels of essential vitamins like thiamine (B1) may also help mitigate the severity of HG. Lifestyle changes, such as eating small, frequent meals high in protein and avoiding spicy, fatty, or oily foods, can be beneficial. However, it is crucial to note that these measures do not guarantee the prevention of HG but can assist in managing and reducing its impact. If you suspect symptoms of HG or have a history of it, consult your healthcare provider promptly.
Diagnosis & Tests
Diagnosing hyperemesis gravidarum (HG) involves a combination of clinical evaluation, medical history, and physical examination. The healthcare provider will assess the severity of the patient's symptoms, such as severe nausea and vomiting of pregnancy that impairs their ability to eat and drink normally, affecting daily activities. These hyperemesis gravidarum symptoms typically begin between the 4th and 6th week of pregnancy and can persist throughout the first trimester or longer. Blood and urine tests may be ordered to check for dehydration, electrolyte imbalances, and ketonuria. Ketonuria may occur due to prolonged starvation, but it is not required for diagnosis; HG is diagnosed clinically based on the severity of nausea/vomiting, inability to maintain hydration/nutrition, weight loss, and functional impairment (RCOG, 2024). The provider may also perform tests to rule out other causes of nausea and vomiting, such as gastrointestinal illnesses or urinary tract infections. An ultrasound may be used to determine if the patient is carrying multiple fetuses or has other conditions like trophoblastic disease, which can also cause HG. Once diagnosed, appropriate hyperemesis gravidarum treatment can be initiated to manage the condition and alleviate the debilitating morning sickness in pregnancy.
Treatment & Management
Managing moderate to severe cases of nausea and vomiting requires medical intervention. Below are key treatment approaches incorporating medications:
1. Prescription Medication
- Doxylamine + Vitamin B6 (Pyridoxine) is often the first-line treatment, helping to reduce nausea and vomiting (RCOG, 2024).
- If symptoms persist, stronger medications such as Promethazine, Metoclopramide, or Ondansetron may be required.
These medications can be administered orally, via injection, or through an IV, depending on the severity of symptoms.
2. IV Fluids
- In cases of dehydration, intravenous (IV) fluids help restore fluid balance and essential nutrients.
- Thiamine supplementation (100 mg IV or oral) should be given before administering IV dextrose or carbohydrate-containing fluids to prevent Wernicke encephalopathy (RCOG, 2024).
3. Tube Feeding
- Enteral feeding (nasogastric or nasojejunal tube) may be considered in refractory cases when oral intake cannot be restored despite optimal medical therapy.
4. IV Nutrition (Total Parenteral Nutrition – TPN)
- Total parenteral nutrition (TPN) is reserved for very severe, refractory cases when both oral and enteral feeding fail. TPN carries significant risks (infection, thrombosis, liver dysfunction) and is not first-line nutritional support.
5. Considerations During Pregnancy
- Some medications carry risks during pregnancy, so it is crucial to consult a doctor before starting any treatment.
Early medical intervention and proper hydration are essential to managing severe nausea and vomiting effectively.
When to See a Doctor?
Consulting a healthcare provider as soon as possible is essential if symptoms of hyperemesis gravidarum are suspected or if there is a history of HG in previous pregnancies. Symptoms that warrant a doctor's consultation include persistent and severe nausea and vomiting that interfere with daily activities and nutrition, weight loss exceeding 5% of pre-pregnancy weight, dehydration indicated by excessive thirst or decreased urine output, electrolyte imbalances identified through blood tests, and psychological distress or significant impact on daily life due to symptoms. If you have a history of HG, discussing your previous experiences and developing a care plan with your healthcare provider before becoming pregnant is advisable. This plan should include pre-emptive treatments such as vitamin B6 supplements and first-line medications for morning sickness. Ensure that your healthcare provider understands your medical history and is prepared to support you with a cohesive hyperemesis gravidarum treatment plan. If symptoms of HG start during pregnancy, seek medical attention promptly, as early treatment can help manage symptoms and prevent complications such as malnutrition, dehydration, and electrolyte imbalances.
Key Takeaways
- HG affects approximately 0.3–3% of pregnancies, depending on diagnostic criteria.
- Symptoms of HG include persistent and severe nausea and vomiting, weight loss, dehydration, and electrolyte imbalances.
- While the exact cause of HG is unknown, it is believed to be related to hormonal changes during pregnancy.
- Treatment for HG may include dietary changes, medications, and, in severe cases, hospitalisation for intravenous fluids and nutrition.
- Although preventing HG with certainty is not currently possible, steps such as taking a multivitamin containing vitamin B6 before pregnancy and maintaining a healthy diet may help reduce the severity of symptoms.
- If symptoms of HG are suspected or there is a history of HG in previous pregnancies, it is essential to consult a healthcare provider promptly for proper diagnosis and treatment.
FAQs
What leads to the development of hyperemesis gravidarum during pregnancy?
What are the treatment options for HG in pregnant women?
Can hyperemesis gravidarum have an impact on the developing baby?
How does hyperemesis gravidarum differ from typical morning sickness?
What is the initial approach to treating hyperemesis gravidarum?
What criteria is used to diagnose hyperemesis gravidarum in pregnant women?
Can hyperemesis gravidarum pose risks to the unborn child?
Are there ways to prevent the onset of hyperemesis gravidarum?
What dietary changes can help alleviate symptoms of hyperemesis gravidarum?
References
- Fejzo, M., Rocha, N., Cimino, I., Lockhart, S. M., Petry, C. J., Kay, R. G., Burling, K., Barker, P., George, A. L., Yasara, N., Premawardhena, A., Gong, S., Cook, E., Rimmington, D., Rainbow, K., Withers, D. J., Cortessis, V., Mullin, P. M., MacGibbon, K. W., … O’Rahilly, S. (2024). GDF15 linked to maternal risk of nausea and vomiting during pregnancy. Nature, 625(7996), 760–767. https://doi.org/10.1038/s41586-023-06921-9
- The Management of nausea and vomiting of pregnancy and hyperemesis gravidarum (Green-Top Guideline No.69) | RCOG. (n.d.). RCOG. https://www.rcog.org.uk/guidance/browse-all-guidance/green-top-guidelines/the-management-of-nausea-and-vomiting-of-pregnancy-and-hyperemesis-gravidarum-green-top-guideline-no-69/?utm
- Jennings, L. K. (2023). Hyperemesis gravidarum. StatPearls. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK532917/
- Vinnars, M. T., et al. (2024). Treatments for hyperemesis gravidarum: systematic review. Acta Obstetricia et Gynecologica Scandinavica / AOGS (systematic review). https://obgyn.onlinelibrary.wiley.com/doi/10.1111/aogs.14706.
Check Related Salts
Latest health articles

Top Health Essentials






























Disclaimer
Top-Selling Medicines:
...View more
Top-OTC medicines:
...View more
Company
About UsHealth ArticleHealth StoriesHealth LibraryDiseases & Health ConditionsAyurvedaUnderstanding Generic MedicinesAll MedicinesAll BrandsNeed HelpFAQSecuritySavings CalculatorAdvertise with UsSubscribe
Registered Office Address
Grievance Officer
Download Truemeds
Contact Us
Our customer representative team is available 7 days a week from 9 am - 9 pm.
v4.28.9
2026 - Truemeds | All rights reserved. Our content is for informational purposes only. See additional information.
Our Payment Partners

