- Medicines
- Personal Care
- Skin Cream
- Sunscreen
- Face Wash
- Skin and Body Soap
- Acne Care
- Body Lotions
- Moisturising Lotion
- Moisturising Cream
- Mosquito Repellent
- Moisturising Gel
- Body Wash
- Hair Oils
- Hair Shampoo
- Hair Conditioners
- Hair Supplements
- Hair Colour
- Hair Serum
- Hair Mask
- Hair Solutions
- Baby Diapers and Wipes
- Baby Lotion and Moisturising Cream
- Baby Bath Essentials
- Baby Skin Care
- Baby and Infant Food
- Baby Healthcare
- Women Multivitamins
- Ovulation Test Kit and Women Intimate Care
- Sanitary Pads
- Nutritional Drinks
- Condoms
- Lubricants
- Massage Gels
- Personal Body Massagers
- Men Performance Booster
- Sexual Health Supplements
- Massage Oils
- Ayurveda
- Tooth Paste
- Mouth Ulcer Gel
- Mouthwash
- Toothache and Gum Pain
- Tooth Brush
- Gargle Solution
- Orthopaedic Supports
- Adult Diapers
- Footwear
- Mobility and Support Accessories
- Urinary Support and Care
- Health Conditions
- Bone and Joint Care
- Digestive Care
- Eye Care
- Pain Relief
- Smoking Cessation
- Liver Care
- Stomach Care
- Cold and Cough
- Heart Care
- Kidney Care
- Piles, Fissures & Fistula
- Respiratory Care
- Mental Wellness
- Derma Care
- Pre and Probiotics
- Acidity
- Gas
- Constipation
- Loose Motion/Diarrhoea
- Digestive Fibres
- Digestive Enzymes
- Eye Lubricant Drops
- Lens Solution
- Safety Eye Wear
- Eye Cream
- Eye Vitamins and Supplements
- Eye Drops
- Eye Ointment and Gel
- Nicotine Patch
- Nicotine Gum
- Nicotine Lozenges
- Cough Syrups
- Chest Rubs and Balms
- Nasal Spray
- Lozenges
- Inhalant Capsules
- Cold and Cough Tablets
- Vitamins & Supplements
- Diabetes Care
- Healthcare Devices
- Homeopathic Medicine
- Health Guide
Prolactinoma
Prolactinoma is a benign tumor of the pituitary gland that produces excessive amounts of the hormone prolactin. It is the most common type of pituitary tumor and can cause symptoms such as infertility, irregular periods, and decreased libido. Treatment options include medication, surgery, and radiation therapy, depending on the size and severity of the tumor.
Last updated on : 16 Dec, 2024
Read time : 16 mins
Overview of Disease
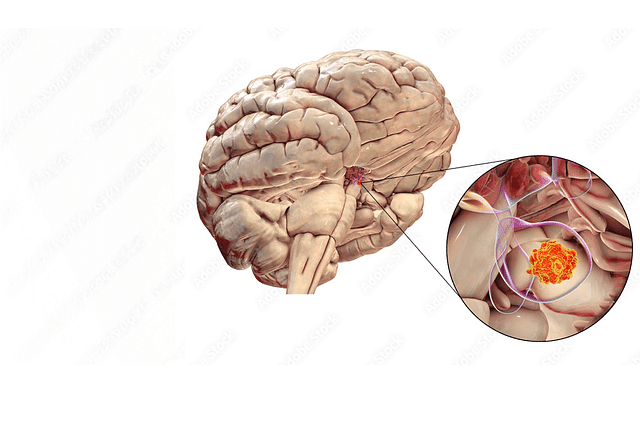
Prolactinoma is a noncancerous tumor that develops in the pituitary gland, a small endocrine gland situated at the base of the brain. The pituitary gland is responsible for regulating various bodily functions, including the production of hormones. Among all pituitary adenomas, prolactinoma is the most prevalent, accounting for roughly 40% of cases. Understanding the nature of prolactinoma is essential for those who may be affected by this condition.
What is Prolactinoma?
Prolactinoma is a tumor that arises from the abnormal growth of lactotroph cells in the pituitary gland, which are responsible for producing the hormone prolactin. Normally, prolactin stimulates milk production in women during pregnancy and breastfeeding. However, in individuals with prolactinoma, the tumor cells secrete excessive amounts of prolactin, leading to a condition called hyperprolactinemia. This hormonal imbalance can cause various symptoms, such as infertility, irregular menstrual periods, and milky nipple discharge in women, as well as erectile dysfunction, decreased libido, and infertility in men.
Although the precise cause of prolactinoma remains unclear, researchers believe that genetic mutations and hormonal imbalances may play a role in its development. In some cases, prolactinoma may be associated with familial syndromes like multiple endocrine neoplasia type 1 (MEN1). As we delve further into the classification of prolactinomas, it becomes evident that their size and secretory nature can significantly impact the presentation and management of this condition.
Key Factors about Prolactinoma
| Category | Details |
| Also Referred as | Pituitary adenoma, Microprolactinoma, Macroprolactinoma |
| Commonly Occurs In | People under age 40, more common in women than men |
| Affected Organ | Pituitary gland |
| Type | Benign (noncancerous) tumour |
| Common Signs | Women: Irregular menstruation, galactorrhoea, infertility, vaginal dryness Men: Erectile dysfunction, low testosterone, infertility Both: Vision problems, headaches, osteoporosis |
| Consulting Specialist | Endocrinologist |
| Treatement Procedures | Medication (dopamine agonists), Surgery, Radiation therapy |
| Managed By | Bromocriptine, cabergoline (dopamine agonists) |
| Mimiciking Condition | Hyperprolactinaemia from other causes (medications, thyroid issues, etc.) |
Types of Prolactinoma
Prolactinomas are primarily classified into two types based on their size:
Microprolactinoma: These are small tumors measuring less than 10 mm in diameter. Microprolactinomas are the most common type of prolactinoma and are often asymptomatic, meaning they may not cause noticeable symptoms.
Macroprolactinoma: These tumors are larger than 10 mm in diameter. Due to their size and location, macroprolactinomas can cause compressive symptoms such as headaches, visual field defects, and cranial nerve palsy.
In some instances, prolactinomas may be further categorized into:
Giant prolactinoma: These tumors exceed 4 cm in diameter and can lead to significant compressive symptoms due to their size.
Mixed tumors: These tumors secrete multiple hormones, including prolactin, and may require a more complex treatment approach.
The classification of prolactinomas based on their size and secretory nature is crucial for determining the most appropriate treatment strategy, which may include medication, surgery, or radiation therapy. By understanding the different types of prolactinomas, healthcare professionals can provide targeted care to manage symptoms and improve patient outcomes.
Symptoms of Prolactinoma
The symptoms of prolactinoma can vary depending on the individual, the size of the tumor, and the levels of prolactin in the body. Some common symptoms include:
Infertility: High prolactin levels can interfere with the production of sex hormones, leading to fertility issues in both men and women.
Bone loss (osteoporosis): Reduced levels of estrogen and testosterone can weaken bones and increase the risk of osteoporosis.
Loss of interest in sexual activity: Both men and women may experience a decrease in libido due to hormonal imbalances caused by the tumor.
In addition to these general symptoms, there are also gender-specific symptoms that can occur.
Symptoms in Women
Women with prolactinoma may experience the following symptoms:
Irregular or absent menstrual periods: High prolactin levels can disrupt the menstrual cycle, causing irregular periods or amenorrhea (absence of menstruation).
Milky discharge from the breasts (galactorrhea): This is a common symptom in women who are not pregnant or breastfeeding.
Painful intercourse: Low estrogen levels can lead to vaginal dryness, causing discomfort during sexual intercourse.
Acne and excessive body and facial hair growth: Some women may experience hirsutism (excessive hair growth) and acne due to hormonal imbalances.
These symptoms can be distressing for women and may have a significant impact on their quality of life. However, prolactinoma treatment can help alleviate these symptoms and restore hormonal balance.
Symptoms in Men
Men with prolactinoma may experience the following symptoms:
Erectile dysfunction: High prolactin levels can cause difficulties in achieving or maintaining an erection, as well as decreased libido.
Decreased body and facial hair: Low testosterone levels can result in reduced body and facial hair growth.
Smaller muscles: Testosterone deficiency can lead to muscle atrophy and decreased muscle mass.
Enlarged breasts (gynecomastia): Elevated prolactin levels can cause breast tissue enlargement in men.
These symptoms may affect a man's self-esteem and confidence. Seeking prompt medical attention and appropriate prolactinoma treatment can help manage these symptoms effectively.
Symptoms Due to Tumor Size and Location
In some cases, the size and location of the prolactinoma can cause additional symptoms, such as:
Vision problems: Large prolactinomas can press on the optic nerve or optic chiasm, causing vision issues like loss of peripheral vision.
Headaches: Pressure from the tumor can lead to headaches, which may be severe or persistent.
Low levels of other pituitary hormones: Larger tumors can compress the healthy part of the pituitary gland, reducing the production of other essential hormones like thyroid hormones and cortisol.
These symptoms can be more severe and may require urgent medical attention. Regular monitoring of the tumor size and hormone levels is crucial for individuals with prolactinoma to prevent complications and ensure timely intervention when necessary.
Stages of Prolactinoma
Prolactinoma has the following stages:
Incubation Period: In the context of prolactinoma, the incubation period is not applicable, as it is a non-infectious condition. However, the development of a prolactinoma can be gradual, and the tumor may grow slowly over time before causing noticeable symptoms. This period can vary significantly among individuals, ranging from months to years.
Prodromal Period: During the prodromal period, the prolactinoma continues to grow, and the patient may begin to experience general symptoms related to elevated prolactin levels. These symptoms can include fatigue, headaches, and mood changes. In women, irregular menstrual cycles or amenorrhea (absence of menstruation) may occur, while men may experience decreased libido or erectile dysfunction.
Illness (Acute) Period: As the prolactinoma progresses, symptoms become more pronounced and specific to the condition. Women may experience galactorrhea (milky discharge from the breasts), infertility, and further menstrual irregularities. Men may develop gynecomastia (enlarged breasts) and a further decline in sexual function. If the tumor grows large enough, it can cause visual disturbances, such as blurred vision or vision loss, due to pressure on the optic nerves.
Treatment Period: Unlike infectious diseases, prolactinoma does not have a natural decline period. Instead, treatment is necessary to manage the condition and reduce tumor size. The primary treatment for prolactinoma is medication, specifically dopamine agonists like cabergoline or bromocriptine. These medications work by reducing prolactin secretion and shrinking the tumor. In some cases, surgery may be required to remove the tumor, particularly if it is large or not responding to medication.
Remission Period: With successful treatment, patients with prolactinoma can enter a remission period. During this stage, symptoms improve, and prolactin levels return to normal. Regular monitoring is essential to ensure that the tumor does not recur and that prolactin levels remain stable. In some cases, long-term medication may be necessary to maintain remission.
Causes of Prolactinoma
The exact cause of prolactinoma remains poorly understood, but several factors and conditions have been identified as potential contributors to the development of this condition.
Genetic Factors: Most prolactinomas occur sporadically, but a small percentage can be attributed to genetic predisposition. Familial cases are rare but can occur as part of multiple endocrine neoplasia type 1 (MEN1) or other familial syndromes.
Hormonal Influence: The exact cause of prolactinoma is not well understood. It is believed to result from genetic mutations that disrupt the normal function of the pituitary gland cells. These mutations lead to uncontrolled growth and prolactin secretion.
Other Factors: Some prolactinomas may be influenced by external factors such as certain medications (e.g., antipsychotics, antidepressants), stress, and thyroid disorders. These factors are not direct causes of the tumor itself but can mimic or exacerbate symptoms.
Understanding the potential role of these factors can help in the diagnosis and management of prolactinoma.
Risk Factors
Prolactinomas are more common in women than in men and are rare in children. Women of reproductive age are more likely to be diagnosed earlier due to symptoms such as irregular menstrual periods, while postmenopausal women and men may be diagnosed later when tumors are larger and cause more noticeable symptoms like headaches and vision problems. Rarely, inherited disorders such as multiple endocrine neoplasia type 1 (MEN1) and familial isolated pituitary adenoma (FIPA) can increase the risk of developing a prolactinoma. However, in most cases, there are no clear risk factors, and the tumors develop sporadically.
Complications
Prolactinomas can lead to several complications if left untreated or not managed properly:
Vision Problems: Large prolactinomas can put pressure on the optic nerves, leading to vision difficulties such as double vision, narrowed field of vision, or even loss of peripheral vision.
Infertility: Excess prolactin can disrupt the reproductive system, leading to hypogonadism. In women, this can cause irregular or no menstrual periods, anovulation, and infertility. In men, it can result in decreased sperm production, erectile dysfunction, and reduced testosterone levels.
Bone Loss (Osteoporosis): The decreased levels of estrogen and testosterone due to high prolactin levels can lead to weakened and brittle bones, increasing the risk of osteoporosis.
Hormonal Imbalance: Large prolactinomas can compress the pituitary gland, interfering with the production and release of other essential hormones such as thyroid hormones and cortisol.
Pregnancy Complications: During pregnancy, the increase in estrogen levels can cause the tumour to grow, leading to symptoms like headaches and vision changes in women with large prolactinomas.
Galactorrhea: The most common symptom is the production of breast milk in men or in women who are not pregnant or breastfeeding.
Addressing these complications is a key focus of prolactinoma treatment. Medication aimed at reducing prolactin levels is often the first line of treatment to alleviate symptoms and prevent further complications.
Prevention of Prolactinoma
While the exact causes of prolactinoma are not fully understood, making prevention challenging, there are some steps that can be taken to reduce the risk of complications associated with this condition. Managing medications that can lead to elevated prolactin levels, such as certain antipsychotics and high blood pressure medications, is one way to help prevent hyperprolactinemia, a key symptom of prolactinomas. For individuals with familial syndromes like multiple endocrine neoplasia type 1 (MEN1), which increases the risk of developing prolactinomas, close monitoring is essential. Regular check-ups and screenings for those with a family history of pituitary tumours can facilitate early detection and timely treatment.
Although prevention may not always be possible, early diagnosis through awareness of prolactinoma symptoms is crucial for effective management and the prevention of long-term complications.
Diagnosis & Tests
Diagnosing a prolactinoma involves a multi-faceted approach:
Physical Exam and Medical History: The first step is a thorough physical examination and a review of the patient's medical history to identify any symptoms or signs that may indicate the presence of a prolactinoma.
Blood Tests: Laboratory tests are conducted to measure the levels of prolactin in the blood. Consistently high prolactin levels are a strong indicator of a prolactinoma. Other hormonal tests may also be performed to assess the functioning of the pituitary gland and to rule out other potential causes for high prolactin levels.
Imaging Tests: If blood tests reveal elevated prolactin levels, imaging tests such as an MRI (magnetic resonance imaging) or CT (computed tomography) scan of the brain are used to visualise the pituitary gland and detect the presence of a tumour. These scans can also help determine the size and location of the tumour.
Visual Field Test: For larger prolactinomas that may be pressing on the optic nerves, a visual field test may be conducted to assess any impact on vision.
A combination of these diagnostic tools allows healthcare professionals to accurately diagnose a prolactinoma and develop an appropriate treatment plan tailored to the individual patient's needs.
Treatment & Management
Treatment options for prolactinoma include medication, surgery, and radiation therapy, depending on the size and severity of the tumor.
Medication: The primary treatment for prolactinoma is medication, specifically dopamine agonists such as bromocriptine and cabergoline. These medications work by reducing the production of prolactin and shrinking the tumor. Dopamine agonists are usually the first line of treatment, as they are effective in controlling prolactin levels and reducing tumor size in most patients. In many cases, medication alone can successfully manage prolactinoma, making it the preferred treatment option.
Surgery: When medication proves ineffective or if the tumor is causing significant problems due to its size or hormone production, surgery may be recommended. The surgical procedure to remove a pituitary tumor is called transsphenoidal surgery, which involves accessing the pituitary gland through the nasal cavity and removing the tumor. Surgery is typically considered when the tumor is large, causing visual disturbances, or not responding to medication. In some cases, surgery may be necessary to obtain a tissue sample for diagnosis.
Radiation Therapy: Radiation therapy is a less common treatment option for prolactinoma and is usually reserved for aggressive or malignant tumors that persist or grow despite medication and surgery. This treatment involves using high-energy radiation to target and destroy tumor cells. Radiation therapy may be used in conjunction with surgery or as a standalone treatment when surgery is not possible or has been unsuccessful. However, radiation therapy is generally not the first choice for treating prolactinoma due to potential side effects and the effectiveness of other treatment options.
Living with Disease
Living with a prolactinoma requires ongoing management and monitoring. Patients often need long-term treatment with dopamine agonists to prevent the tumor from growing back. Regular follow-up appointments with an endocrinologist are crucial to monitor prolactin levels and tumor size. If the tumor shrinks significantly and prolactin levels remain normal for at least two years, the medication may be tapered off under medical supervision. However, prolactin levels can rise again after stopping the medication, necessitating its restart. During pregnancy, special precautions are needed, and close collaboration between the endocrinologist and obstetrician is essential to ensure the safety of both the mother and the developing fetus. Emotional support from family, friends, and support groups can be invaluable in coping with the challenges of living with a prolactinoma.
When to See a Doctor?
It is important to consult a healthcare professional if you experience symptoms suggestive of a prolactinoma, such as persistent headaches, vision changes, irregular menstrual cycles, infertility, or milky nipple discharge (galactorrhea). These symptoms may also be caused by other conditions, so a proper diagnosis is crucial. If you have been diagnosed with a prolactinoma, you should see your endocrinologist regularly for monitoring of your prolactin levels and tumor size. Any changes in your symptoms, such as worsening headaches or vision problems, should prompt an immediate medical evaluation. Additionally, if you are planning to become pregnant or are currently pregnant, it is essential to discuss your condition with your healthcare provider to ensure appropriate management and monitoring throughout your pregnancy.
Key Takeaways
Prolactinomas are benign tumors of the pituitary gland that cause excess production of prolactin hormone
Common prolactinoma symptoms include irregular menstrual periods, infertility, and milky discharge from the breasts in women, and low libido, erectile dysfunction, and infertility in men
Prolactinomas are usually diagnosed through blood tests measuring prolactin levels and brain imaging scans like MRI
Treatment for prolactinomas typically involves medications called dopamine agonists, such as cabergoline and bromocriptine, which reduce prolactin production
Surgery to remove the tumor may be considered if medications are ineffective or not tolerated, or if the tumor is very large and pressing on surrounding brain structures
Regular monitoring with blood tests and periodic MRI scans is important to assess treatment response and check for any tumor regrowth
With appropriate prolactinoma treatment, symptoms usually improve and the tumor often shrinks in size, allowing restoration of regular menstrual cycles and fertility in women
Most people with prolactinomas have an excellent prognosis and are able to lead normal lives with medical therapy; the medications are generally well-tolerated and effective in controlling the disease
FAQs
What exactly is a prolactinoma?
A prolactinoma is a non-cancerous tumor of the pituitary gland that secretes the hormone prolactin. It is a benign growth, not a brain tumor.
Is it possible to cure a prolactinoma completely?
Prolactinomas can be managed effectively with treatment. Medications can control prolactin levels and shrink the tumor in most cases, while surgery may be necessary for larger tumors.
What are the common symptoms experienced with a prolactinoma?
Prolactinoma symptoms include infertility, menstrual irregularities, galactorrhea, reduced libido, erectile dysfunction, gynecomastia, osteoporosis, vision problems, and headaches, varying based on tumor size and gender.
What are the signs of elevated prolactin levels?
High prolactin levels can cause infertility, menstrual irregularities, galactorrhea, reduced libido, erectile dysfunction, gynecomastia, osteoporosis, vision problems, and headaches.
What causes high prolactin levels in unmarried women?
Prolactin levels can be elevated due to various factors, including pregnancy, nipple stimulation, stress, certain medications, hypothyroidism, and benign conditions like macroprolactinemia, regardless of marital status.
Can a prolactinoma be malignant?
Prolactinomas are typically benign tumors and are not cancerous.
What are some natural ways to lower prolactin levels?
Natural methods to reduce prolactin may include stress reduction, regular exercise, maintaining a healthy diet, and avoiding excessive nipple stimulation. However, medical intervention is often necessary for prolactinomas.
How quickly do prolactinomas typically grow?
The growth rate of prolactinomas varies depending on the individual. Some may remain stable for years, while others may grow more rapidly. Regular monitoring is essential.
Is it possible for high prolactin levels to return to normal?
Yes, with appropriate treatment, such as dopamine agonist medications, prolactin levels can often be restored to normal range.
Can stress contribute to the development of a prolactinoma?
While stress can cause a temporary increase in prolactin levels, it is not a direct cause of prolactinomas. The exact causes of prolactinomas are not fully understood, but genetic factors may play a role.
References
Glezer, A., & Bronstein, M. D. (2015). Prolactinomas. Endocrinology and Metabolism Clinics of North America, 44(1), 71-78. https://doi.org/10.1016/j.ecl.2014.11.003
Klibanski, A. (2010). Clinical practice. Prolactinomas. The New England Journal of Medicine, 362(13), 1219–1226. https://doi.org/10.1056/NEJMcp0912025
Langlois, F., McCartney, S., & Fleseriu, M. (2017). Recent progress in the medical therapy of pituitary tumors. Endocrinology and Metabolism (Seoul, Korea), 32(2), 162–170. https://doi.org/10.3803/EnM.2017.32.2.162
Melmed, S., Casanueva, F. F., Hoffman, A. R., Kleinberg, D. L., Montori, V. M., Schlechte, J. A., & Wass, J. A. (2011). Diagnosis and treatment of hyperprolactinemia: An endocrine society clinical practice guideline. The Journal of Clinical Endocrinology and Metabolism, 96(2), 273–288. https://doi.org/10.1210/jc.2010-1692


Check Related Salts
Browse Other Conditions
Latest health articles








Top Health Essentials
































Disclaimer
Top-Selling Medicines:
...View more
Top-OTC medicines:
...View more
Subscribe
Registered Office Address
Grievance Officer
Download Truemeds
Contact Us
Our customer representative team is available 7 days a week from 9 am - 9 pm.
v3.7.5
Our Payment Partners

